







Pearl is a clinical professor of plastic surgery at the Stanford University School of Medicine and is on the faculty of the Stanford Graduate School of Business. He is a former CEO of The Permanente Medical Group.
During my residency at Stanford, I traveled to Mexico with a group of surgeons to operate on children with cleft lips and palates. On the first day, I watched in awe as the team leader meticulously realigned the tissues of the lip, mouth and nose of a 3-month-old boy, leaving behind nothing but a faint scar — all in just 90 minutes.
I immediately fell in love with plastic and reconstructive surgery. As a surgeon, I visited over a dozen countries to repair the cleft lips and palates of children. But later, in my leadership role as CEO at Kaiser Permanente, extended travel proved impossible. And I missed those trips dearly.
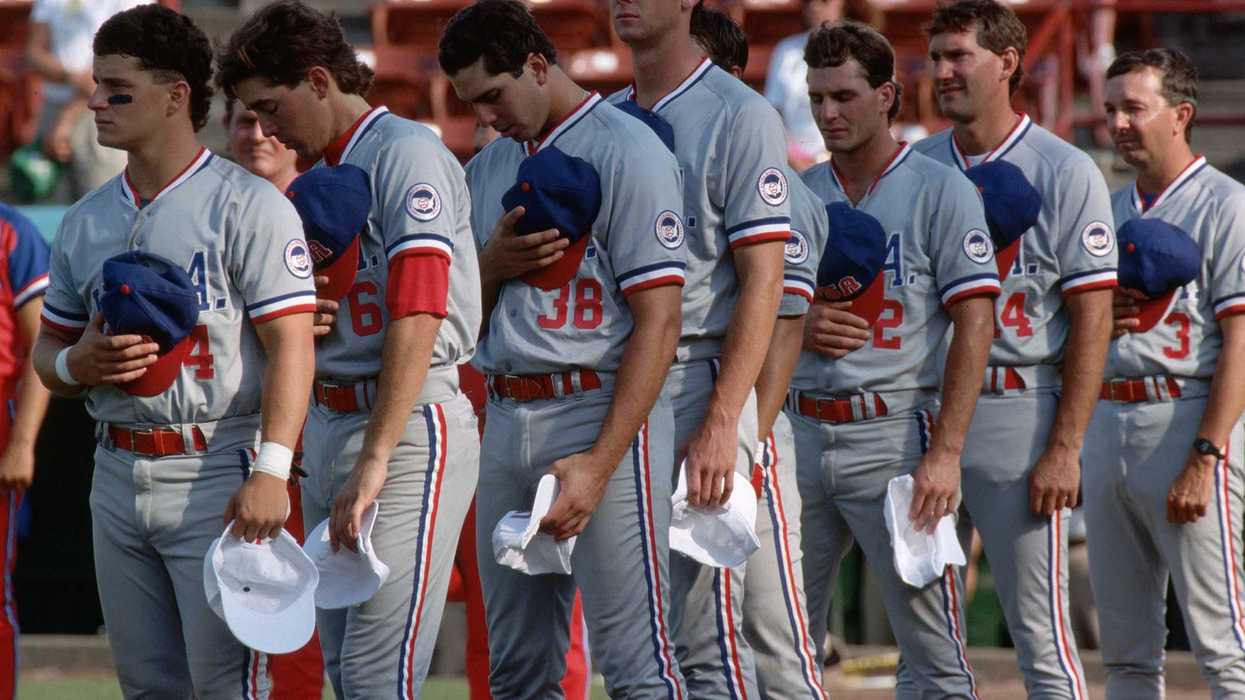
Last month marked my first global surgery mission in many years. Not only did our time in the Philippines reignite my passion for global surgery, but it also left me with three surprising lessons for American health care:
Without mission and purpose, medicine proves exhausting
Surgical trips are physically and emotionally demanding. Far from the sterilized corridors of American hospitals, you are plunged into environments where resources are scarce and the needs overwhelming. In remote towns and underdeveloped cities, you operate in tight spaces with erratic electricity and limited clean water. The days stretch long, with five to seven surgeries in a 12-hour day.
Each child you treat carries a story of hardship and hope, their families’ eyes filled with a mix of fear and optimism. And just as you start to tire from the heat and yearn for a good night’s sleep, another mother arrives. She has walked for two days through the mountains with a child in her arms, praying her baby can be added to the surgical schedule. There is no saying “no” to this. You immediately become reinvigorated.
After a physically trying week, you return to the United States not exhausted, but emotionally replenished. Nearly every clinician who has participated in a surgical mission feels the exact same way.
American health care today obscures the fundamental mission and purpose that motivates clinicians. Physicians find themselves ensnared in a web of administrative tasks and insurance disputes. For many doctors, this noble calling has become just a job.
To revive the profession and address the burnout crisis that affects more than 60 percent of clinicians, a renaissance of purpose is imperative.
To get there, we must pivot away from the transactional “fee for service” financial model that rewards doctors for the sheer quantity of services rendered. In its place: a reimbursement model led by clinicians who are paid based on the quality of clinical outcomes achieved.
Inherent in the privilege of healing is the duty to lead this transformation. Taking on that accountability — and thereby eliminating the care restrictions that insurance companies impose — will rejuvenate, not further fatigue, health care professionals.
American doctors are excellent but so are physicians around the globe
U.S. physicians believe that training outside the States is a second-rate education. It’s time to alter that perspective.
During my week in the Philippines, I had the pleasure to work alongside five local physicians, often at adjoining operating room tables. They’d trained in residency and fellowship programs all around the world to maximize their expertise. To a person, their results matched the leading pediatric hospitals in the United States.
Although American doctors have access to the best facilities, machines and materials, physicians in other nations have a competitive advantage that comes from higher volume. The best way to hone any medical skill is through repetition and experience. American surgeons lag their global colleagues in this area.
U.S. clinicians bring a wealth of knowledge that can greatly benefit doctors worldwide, yet there are equally rich lessons to learn from the experiences and practices of physicians abroad.
In the U.S. today, doctors adhere to minimum surgical volume standards. Patient outcomes would improve tremendously if, instead, our nation set benchmarks for superior performance. Combining high-volume surgical experience with our advanced technologies and top-notch facilities would produce superlative clinical outcomes.
But first, America’s health care professionals need to embrace humility and be open to learning from our global colleagues.
U.S. resources are vast but access is still scarce
In countries like the Philippines, health care challenges are magnified by economic constraints. Despite government coverage, per capita health care spending remains low, under $200 annually. This financial reality forces difficult choices, leaving significant gaps between the health care needs of the population and the services available.
Witnessing these disparities firsthand is a poignant reminder of the abundance the United States enjoys, with health care spending now exceeding $13,000 per American. And yet, despite our nation’s wealth, independent studies reveal that U.S. health care ranks last among a dozen wealthy nations and near the bottom of 38 OECD countries in more than a dozen health measures.
The United States has earned its distinction as home to the most expensive and least effective health care system in the developed world. This isn’t just because of our 30 million uninsured citizens (and tens of millions who are underinsured). It’s the result of decades of underinvestment in primary care, tolerance of inefficient hospital systems and exorbitant drug prices.
The challenge of transforming American health care is daunting, and it requires a willingness to embrace change and confront uncomfortable truths. Observing the efficiency and ingenuity of less affluent nations inspires a reevaluation of our own care-delivery practices and health care finances.
The biggest problem in our health care system isn’t a lack of money. It’s the deficit in leadership and innovation.
Volunteering on global missions offers invaluable perspectives that could catalyze change in the United States. I’m optimistic that by learning from countries that achieve remarkable outcomes with modest means, we can enhance clinical outcomes, reduce clinician burnout, and make quality health care accessible and affordable for all Americans.











A golden tray sits on the Resolute Desk as President Donald Trump speaks during an announcement on American nuclear innovation in the Oval Office at the White House on July 24, 2026, in Washington, D.C. Trump is signing multiple executive orders targeting the nuclear energy sector and easing rules for new reactors and nuclear fuel supply chains.
Trump’s hubris rivals the fallen heroes of ancient Greek mythology
In January, the New York Times asked President Donald Trump if there were any limits on his global powers.
“Yeah,” the president responded, “there is one thing. My own morality. My own mind. It’s the only thing that can stop me.”
That was eight months ago, but fortunately Christopher Nolan’s blockbuster adaptation of “The Odyssey” has made ancient Greek literature newly relevant. Before that window closes, I’d like to talk about hubris.
Today, the term mostly means excessive pride or arrogance. That’s part of what the Greeks meant by it too, but the meaning was a bit richer and more specific. Hubris was an insolent or outrageous act that offended the gods, often because the transgressor was claiming abilities or authorities that solely belonged to supreme beings.
Nolan renamed and slightly modified the concept of xenia for the film, calling it “Zeus’ law.” In the director’s telling, mortals should follow the rules laid out by the gods, specifically the requirement to treat strangers with respect lest they be gods in disguise.
In a sense, hubris is the opposite, or at least the rejection, of xenia. The hubris of the suitors, and at times Odysseus himself, invites punishment by the gods and their mortal instruments.
Which brings me back to Donald Trump. His claim that there are no constraints on his personal power to dictate events on the global stage was one of the greatest expressions of hubris ever uttered by a political leader.
Trump’s claim was obviously false when he made it.
He vowed that he could end the Russia-Ukraine war in 24 hours. He’s proved powerless to make that happen. If he had divine powers to work his will, why would he have balked at implementing his tariffs so often that Wall Street adopted the “TACO trade” term for his deals? “TACO” stands for “Trump always chickens out.”
And why would Trump have made so many embarrassing concessions to China — from rescinding tariffs on Chinese goods to allowing them to buy crucial and incredibly valuable computer chips?
But Trump saw his success at capturing Venezuelan strongman Nicolas Maduro as proof of his ability to launch missiles to the same effect as Zeus’ lightning bolts. Trump believed he was the most powerful man who ever lived.
This is no exaggeration. In March, when the Iran invasion seemed successful, Trump gave a document penned by“Presidential Historian David King” to New York Times reporters Maggie Haberman and Jonathan Swan purporting to prove that Trump was “the most powerful person to have EVER walked this planet.” King was, in fact, a businessman and occasional caddy for legendary golfer Gary Player.
King compared Trump favorably to many of history’s most powerful, and often heinous, figures: Alexander the Great, Attila the Hun, William the Conqueror, Napoleon Bonaparte, Joseph Stalin, Genghis Khan, Mao Tse Tung, Adolf Hitler and Vladimir Lenin. Many of these men thought they were the most powerful person in the world, too. And many were defeated precisely because they believed it.
At least Napoleon and Hitler had a string of truly impressive victories before they learned the folly of hubris. The limits on Trump’s power have been exposed by far less august forces than the combined might of the allies in World War II or the fearsome Russian winter.
Iran is a comparatively middling power. But the regime’s ability to absorb punishment while imposing its will on the Strait of Hormuz has proved to be a greater constraint on Trump’s power than his morality or mind. We should note that, at least rhetorically, his morality has not proved much of a constraint. He has repeatedly promised to destroy Iranian “civilization” if the regime refuses to capitulate.
But they haven’t — and won’t anytime soon — because the regime’s tolerance for pain far outstrips Trump’s. The combined fear of skyrocketing oil prices, outrage of Gulf state potentates, diminishing weapon supplies and domestic unpopularity is doing the work that international law, congressional oversight and the collective opinion of foreign policy experts can’t or won’t do.
If I considered Trump more heroic than reason and facts could allow, I would say his Sisyphean predicament has the whiff of Greek tragedy to it. Trump is vexed by the fact that the Iranians won’t honor deals or ratify his countless premature claims of victory — giving new meaning to his vow that his presidency would make people tired of winning. It’s almost like they’re out-Trumping Trump.
Things might have gone better if he’d heeded that great Greek tragedian Sophocles: “For Zeus utterly abhors the boasts of a proud tongue.”
____
Jonah Goldberg is editor-in-chief of The Dispatch and the host of The Remnant podcast. His Twitter handle is @JonahDispatch.