







Why does The Fulcrum feature regular columns on health care in America?
U.S. health care spending grew 9.7 percent in 2020, reaching $4.1 trillion — 19.7 percent of the gross domestic product. Over the long term this is clearly unsustainable. If The Fulcrum is going to fulfill our mission as a place for informed discussions on repairing our democracy, we need to foster conversations on this vital segment of the economy. Maximizing the quality and reducing the cost of American medicine not only will make people's lives better, but will also generate dollars needed to invest in education, eliminating poverty or other critical areas. This series on breaking the rules aims to achieve that goal and spotlights the essential role the government will need to play.
Pearl is a clinical professor of plastic surgery at the Stanford University School of Medicine and is on the faculty of the Stanford Graduate School of Business. He is a former CEO of The Permanente Medical Group.
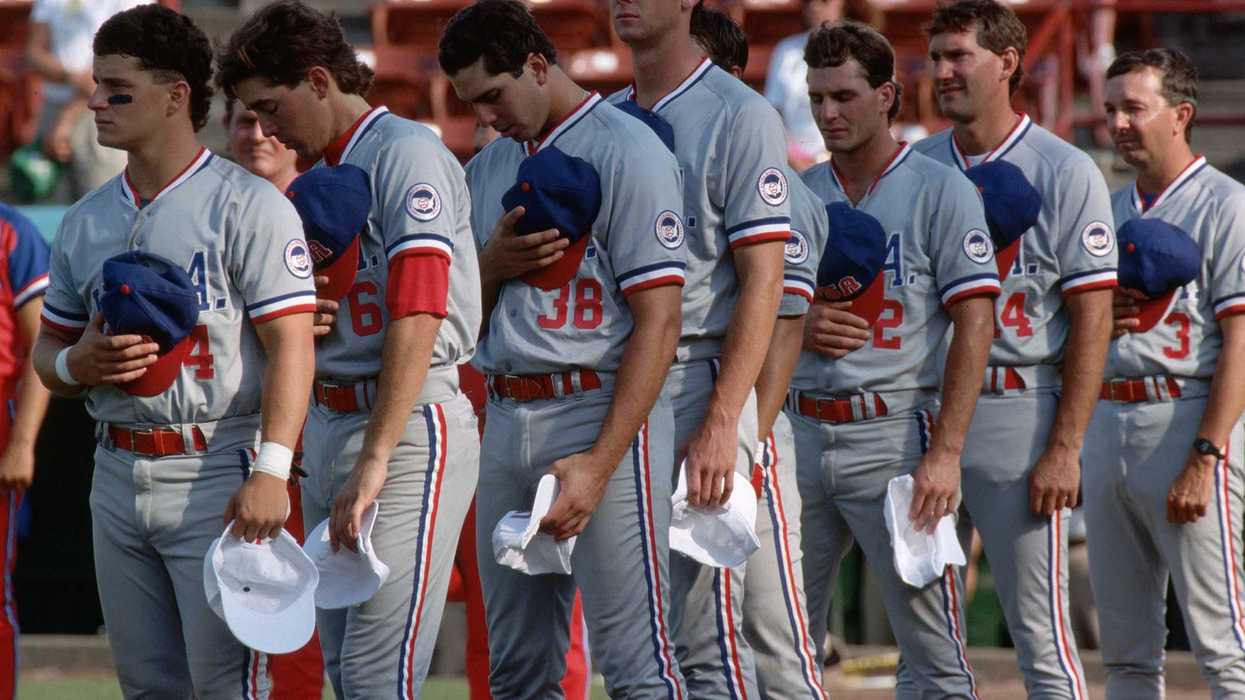
Prior to the pandemic, the richest people in the United States lived nearly 15 years longer than the poorest Americans.
Without quick and radical intervention, that gap will get much wider.
Rising inflation, which hit a 40-year high in 2022, will devastate the health of the low-income Americans by delivering a 1-2-3-punch combination.
Punch 1: Initial hit to personal health
When it comes to nutrition, impoverished Americans experience a different set of problems than impoverished people in developing nations. The distinction is what researchers call the obesity-poverty paradox.
In U.S. households where families earn less than $45,000 per year, the obesity rate is above 35 percent. That’s 10 percent higher than in homes with median incomes over $65,000.
When Americans have less money for ( or access to) healthy foods, there’s little choice but to eat cheap, high-calorie meals with minimal nutritional value. Inflation is already exacerbating this problem for low-income families, elevating their risk for obesity-associated illnesses like hypertension, diabetes, heart disease and cancer.
Punch 2: Delayed hit to health care access
Few Americans understand how medical pricing works, which is why most people won’t see this next punch coming.
Even the media underestimate the threat, as this recent headline from CNN demonstrates: “Prices are soaring but not for health care.”
While that’s true so far, the fact is that health care prices don’t fluctuate in real-time as with groceries or gas.
Health insurers negotiate contracts with doctors, hospitals and drug manufacturers on an annual basis. Most of them haven’t yet renewed. But when the next insurance pricing cycle arrives in early 2023, higher medical spending will hit patients in the form of sharply rising out-of-pocket expenses.
For low- and middle-income families who are already struggling to afford medications like insulin and to pay their hospital bills (which are the leading cause of bankruptcy in the United States), this second punch will hurt for years.
Punch 3: Crushing blow of chronic disease
People who can’t afford healthy foods, medications or doctor visits are more prone to developing chronic illnesses (heart disease, diabetes, asthma, etc.), often more than one.
Chronic medical conditions account for seven in 10 deaths today and have caused national life expectancy to plateau over the past two decades. Inflation will make it worse.
Chronic diseases not only sap people’s health but their finances, too. They result in missed work, which reduces earning potential, creating a vicious cycle in which people need more medical care but can’t afford it.
Following the one-two combination of poorer nutrition and restricted health care access, rising rates of chronic illness will be the body blow that low-income Americans feel for decades.
Winning the fight by changing the game
American health is influenced by much more than just medical treatments. Individual behaviors and societal factors like housing and education have been shown to contribute greatly.
But better medical care would make a tremendous difference in the lives of low-income patients, and it is attainable if we change a) the way doctors deliver care and b) how they’re paid for it.
Doing so would help our nation defeat a daunting health care enemy: wasted spending.
Each year, Americans throw away $1 trillion on duplicate medical tests, ineffective treatments and failures of care coordination. One way to weed out waste is to bring physicians and hospitals together (to form “ integrated health systems ”). With better coordination and teamwork, these multispecialty medical groups have been shown to reduce redundant services, prevent chronic diseases and keep low-income patients from slipping through the cracks of the system.
But, in addition to integrating care delivery, we must fix the broken health care payment model and erase its perverse incentives.
Today, health insurers reimburse doctors on a “fee for service” basis, paying them for each new test and treatment, even when these services fail to help. A better approach involves prepaying for health care, which flips physician incentives around. When doctors are paid a lump-sum, in advance, to satisfy all the medical needs of a group of patients for an entire year, the focus shifts from the quantity of care they provide to the quality.
Unfortunately, Congress has done little over the last decade to advance these changes. With the growing partisan divide on Capitol Hill, we can’t assume it’ll happen anytime soon. Therefore, amid rising inflation, the best way to meet the medical needs of low-income Americans will be to bypass the legislative process, altogether.
Today, patients enrolled in Medicare Advantage, through Medicaid Managed Care Organizations and via the HealthCare.gov marketplace, already take part in prepaid insurance arrangements. But there’s a catch: Instead of the government prepaying physicians (or integrated systems) directly, contracts are awarded to insurance companies, which most often pay health care providers on a fee-for-service basis.
So, if the Centers for Medicare & Medicaid Services wants to help eliminate wasted dollars and align incentives for doctors, the agency will need to allow integrated systems to compete with insurers for prepaid contracts. This change can be administered by HHS unilaterally without relying on a lengthy and partisan battle in Congress.
The winners would then need to work in close collaboration with other governmental agencies and organizations to assist in improving the health of low-income patients.
For example, using data obtained from existing Medicare and Medicaid providers, CMS could publish a list of the medical services that are most helpful vs. most wasteful. This information would be used to improve the care of patients, evaluate the annual performance of each integrated system and serve as the comparative basis for contract renewals the following year.
Also, since access to food is proven to promote healthier eating and reduce the incidence of chronic illness, the Department of Health and Human Services could earmark discretionary funds for “healthy eating stipends” in partnership with the Department of Agriculture’s Food and Nutrition Service. When referred by a physician, low-income families could use these stipends to offset the higher cost of healthier foods.
Finally, to provide better care at lower costs, doctors will need to embrace modern technologies. These include telehealth, home-monitoring devices, data analytics and artificial intelligence. To boost adoption, the Health Information Technology agency within HHS would assist newly formed integrated health systems with implementing the medical technologies proven to be most effective, rather than the multimillion-dollar gadgets that fail to improve health outcomes.
CMS Administrator Chiquita Brooks-LaSure could work with leaders from the Office of the National Coordinator for Health Information Technology to ensure low-income Americans obtain the health benefits technology offers.
To bolster our nation’s health and defend Americans against inflation, we need to reduce wasteful spending in our medical system. Wealthy Americans have the resources to pay for overpriced, ineffective health care. But amid rising inflation, low-income Americans cannot. The best way to win the fight is to change how doctors deliver care and get paid for it. We can do it with the help of existing government agencies.











A golden tray sits on the Resolute Desk as President Donald Trump speaks during an announcement on American nuclear innovation in the Oval Office at the White House on July 24, 2026, in Washington, D.C. Trump is signing multiple executive orders targeting the nuclear energy sector and easing rules for new reactors and nuclear fuel supply chains.
Trump’s hubris rivals the fallen heroes of ancient Greek mythology
In January, the New York Times asked President Donald Trump if there were any limits on his global powers.
“Yeah,” the president responded, “there is one thing. My own morality. My own mind. It’s the only thing that can stop me.”
That was eight months ago, but fortunately Christopher Nolan’s blockbuster adaptation of “The Odyssey” has made ancient Greek literature newly relevant. Before that window closes, I’d like to talk about hubris.
Today, the term mostly means excessive pride or arrogance. That’s part of what the Greeks meant by it too, but the meaning was a bit richer and more specific. Hubris was an insolent or outrageous act that offended the gods, often because the transgressor was claiming abilities or authorities that solely belonged to supreme beings.
Nolan renamed and slightly modified the concept of xenia for the film, calling it “Zeus’ law.” In the director’s telling, mortals should follow the rules laid out by the gods, specifically the requirement to treat strangers with respect lest they be gods in disguise.
In a sense, hubris is the opposite, or at least the rejection, of xenia. The hubris of the suitors, and at times Odysseus himself, invites punishment by the gods and their mortal instruments.
Which brings me back to Donald Trump. His claim that there are no constraints on his personal power to dictate events on the global stage was one of the greatest expressions of hubris ever uttered by a political leader.
Trump’s claim was obviously false when he made it.
He vowed that he could end the Russia-Ukraine war in 24 hours. He’s proved powerless to make that happen. If he had divine powers to work his will, why would he have balked at implementing his tariffs so often that Wall Street adopted the “TACO trade” term for his deals? “TACO” stands for “Trump always chickens out.”
And why would Trump have made so many embarrassing concessions to China — from rescinding tariffs on Chinese goods to allowing them to buy crucial and incredibly valuable computer chips?
But Trump saw his success at capturing Venezuelan strongman Nicolas Maduro as proof of his ability to launch missiles to the same effect as Zeus’ lightning bolts. Trump believed he was the most powerful man who ever lived.
This is no exaggeration. In March, when the Iran invasion seemed successful, Trump gave a document penned by“Presidential Historian David King” to New York Times reporters Maggie Haberman and Jonathan Swan purporting to prove that Trump was “the most powerful person to have EVER walked this planet.” King was, in fact, a businessman and occasional caddy for legendary golfer Gary Player.
King compared Trump favorably to many of history’s most powerful, and often heinous, figures: Alexander the Great, Attila the Hun, William the Conqueror, Napoleon Bonaparte, Joseph Stalin, Genghis Khan, Mao Tse Tung, Adolf Hitler and Vladimir Lenin. Many of these men thought they were the most powerful person in the world, too. And many were defeated precisely because they believed it.
At least Napoleon and Hitler had a string of truly impressive victories before they learned the folly of hubris. The limits on Trump’s power have been exposed by far less august forces than the combined might of the allies in World War II or the fearsome Russian winter.
Iran is a comparatively middling power. But the regime’s ability to absorb punishment while imposing its will on the Strait of Hormuz has proved to be a greater constraint on Trump’s power than his morality or mind. We should note that, at least rhetorically, his morality has not proved much of a constraint. He has repeatedly promised to destroy Iranian “civilization” if the regime refuses to capitulate.
But they haven’t — and won’t anytime soon — because the regime’s tolerance for pain far outstrips Trump’s. The combined fear of skyrocketing oil prices, outrage of Gulf state potentates, diminishing weapon supplies and domestic unpopularity is doing the work that international law, congressional oversight and the collective opinion of foreign policy experts can’t or won’t do.
If I considered Trump more heroic than reason and facts could allow, I would say his Sisyphean predicament has the whiff of Greek tragedy to it. Trump is vexed by the fact that the Iranians won’t honor deals or ratify his countless premature claims of victory — giving new meaning to his vow that his presidency would make people tired of winning. It’s almost like they’re out-Trumping Trump.
Things might have gone better if he’d heeded that great Greek tragedian Sophocles: “For Zeus utterly abhors the boasts of a proud tongue.”
____
Jonah Goldberg is editor-in-chief of The Dispatch and the host of The Remnant podcast. His Twitter handle is @JonahDispatch.